.jpeg)
Table of Contents
GLP-1 medications (semaglutide and tirzepatide, sold as Ozempic, Wegovy, and Mounjaro) are now among the most prescribed drugs in the country. Among commercially insured adults, use jumped from 3.7% in 2019 to 16.5% in 2024. In five years, the patient population walking into orthopedic practices changed shape.
The weight loss is real. The benefits are real. The downstream musculoskeletal consequences are real too, and almost nobody is watching them.
GLP-1 is doing exactly what it was designed to do. The gap opens after. Patients drop weight fast, and no structured orthopedic support is tracking what that speed costs their muscle, bone, and joints.
What the research shows
Start with muscle. In the STEP 1 trial of semaglutide, 38% of the total weight patients lost was lean body mass, which is mostly muscle. That's about 5.3 kg out of an average 13.6 kg lost. Without structured resistance training, muscle can account for 20 to 25% of total weight lost in men and 10 to 15% in women.
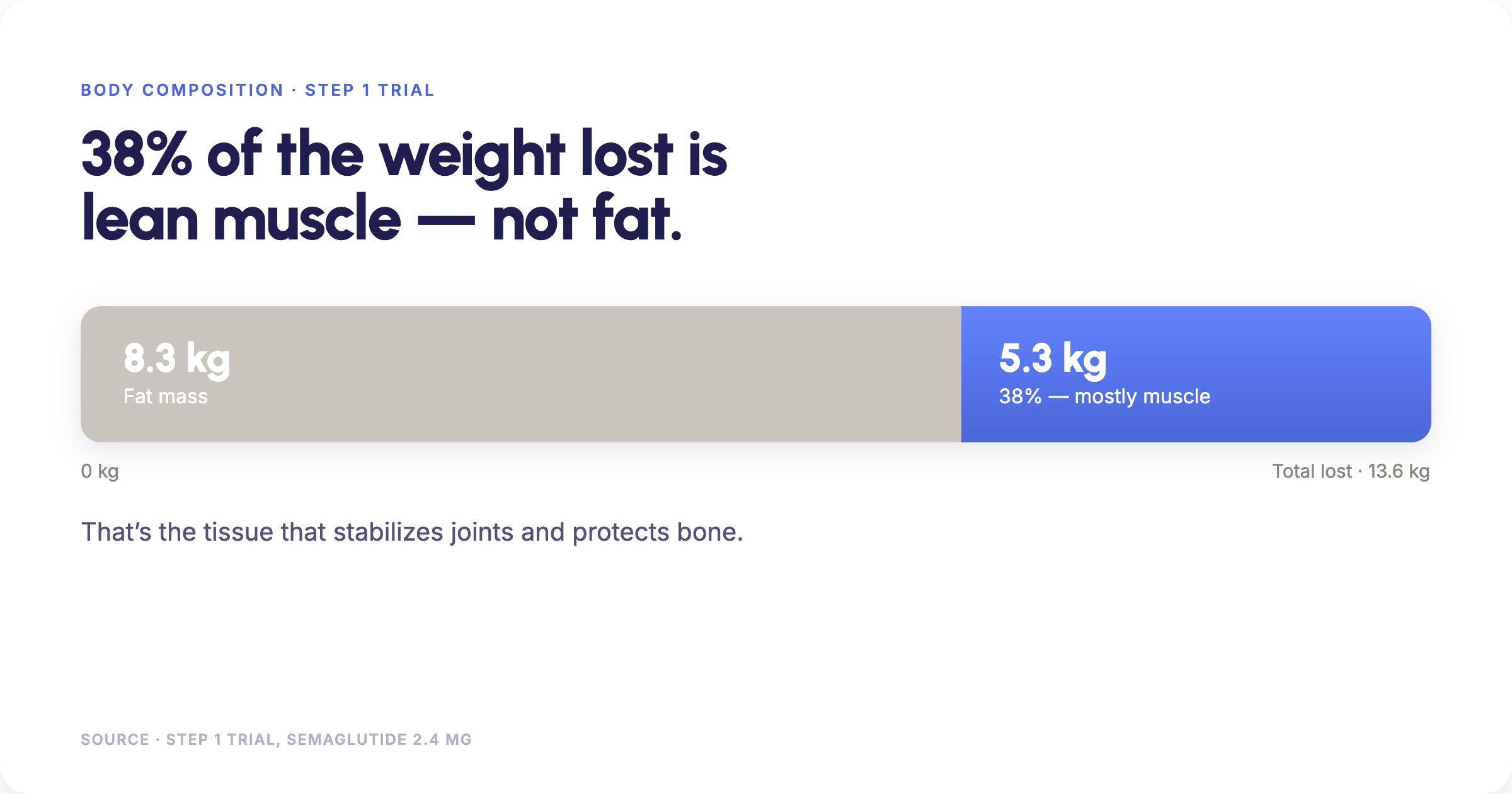
That is the tissue that stabilizes joints, protects bone, and keeps people functional. Losing a quarter of it is not a cosmetic problem.
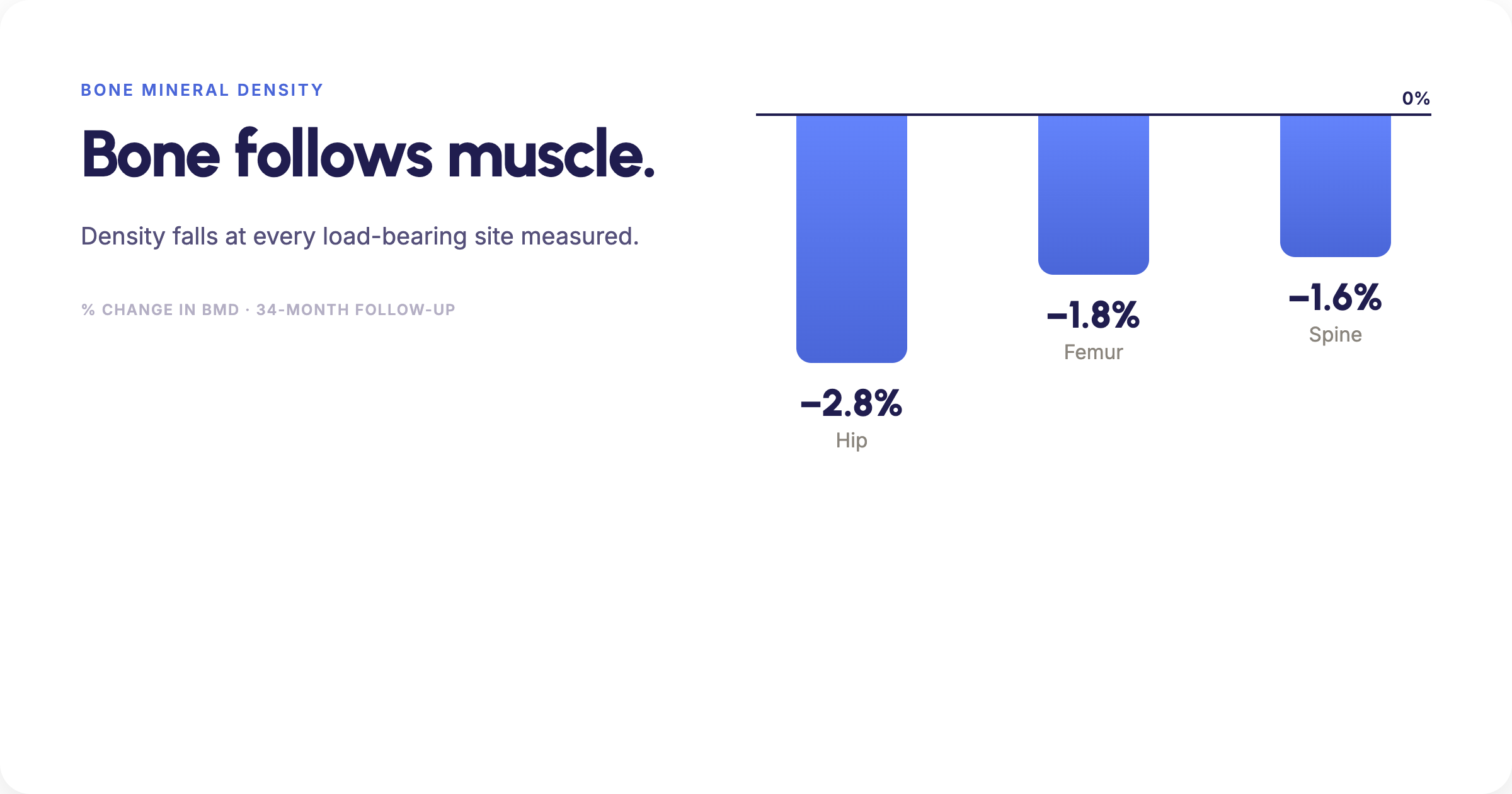
Bone follows muscle. Studies of semaglutide and tirzepatide found meaningful drops in bone mineral density, the standard measure of bone strength: down 2.8% at the total hip, 1.8% at the femoral neck, and 1.6% at the lumbar spine over an average 34-month follow-up. In non-diabetic patients, total hip bone loss was greater on GLP-1 (-1%) than in matched controls (-0.6%) over 17 months. The more weight a patient lost, the more bone they lost with it (r = 0.32, P < .01).
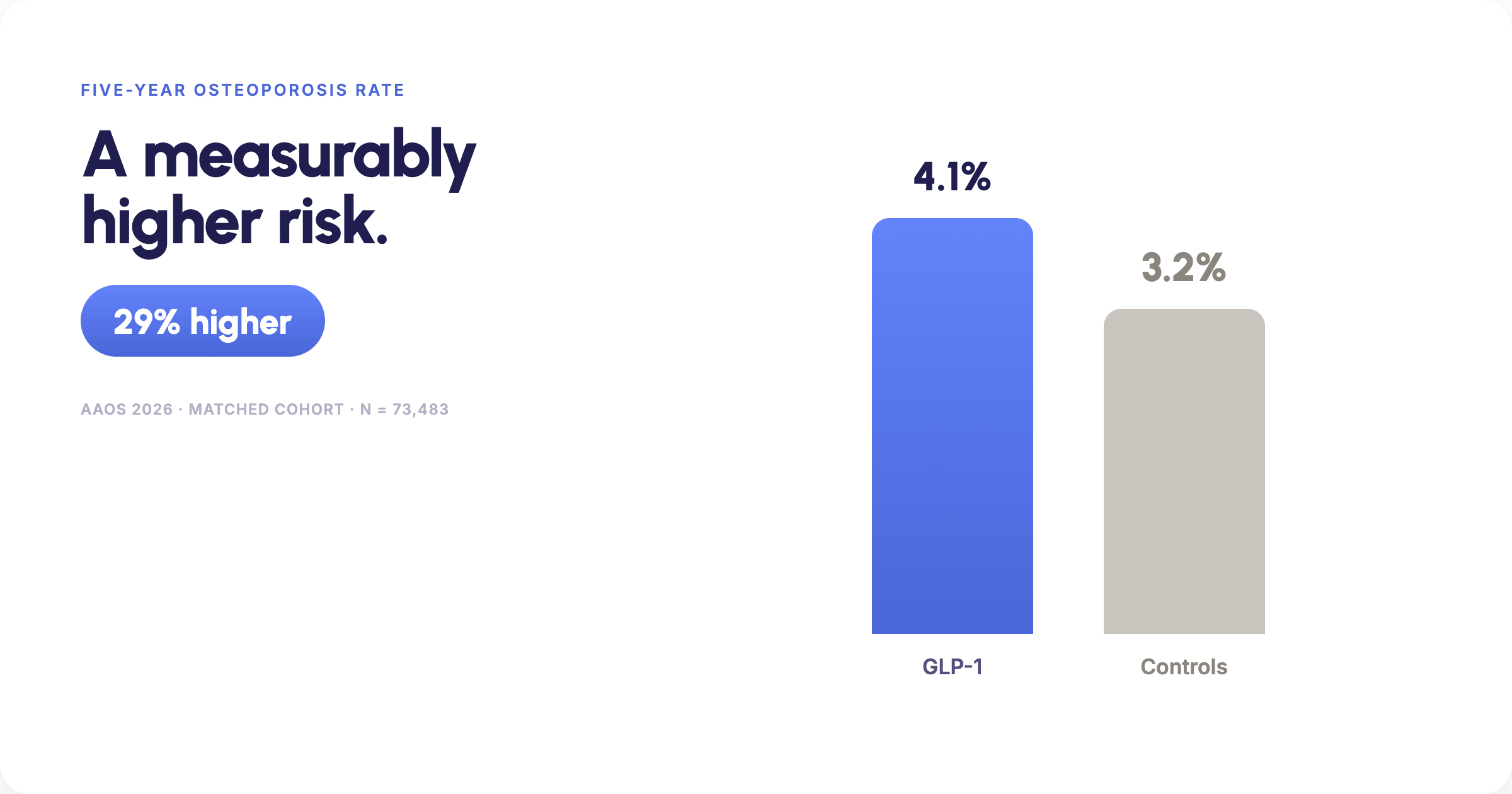
Then the outcome that matters. At the AAOS 2026 Annual Meeting, a matched cohort of 73,483 patients showed a 5-year osteoporosis rate of 4.1% among GLP-1 users versus 3.2% in controls (RR 1.29, p < 0.001). That is a 29% higher rate of osteoporosis.
These are already your patients
Here is the part that's easy to miss. This is not a new patient population arriving from somewhere else.
16.5% of commercially insured adults. That is roughly one in six. Do the math on your own panel.
And they did not arrive at a GLP-1 by accident. Most came to it through obesity and metabolic disease, the same conditions that put a patient in an orthopedic waiting room eventually anyway. The osteoporosis signal above lands in a group that was already carrying elevated musculoskeletal risk before the first dose.
Rapid weight loss did not create that risk. It rearranged it, on a timeline nobody is tracking.
So the question for a practice isn't whether these patients are coming. They are already on your schedule, already in your community, and already changing underneath you. The question is whether anyone will notice the change before it becomes a diagnosis.
The specialist who was never in the room
Muscle and bone are orthopedics. That is the whole specialty.
So it is worth asking, plainly: who is the orthopedic specialist involved in the maintenance of a GLP-1 patient?
For almost all of them, the answer is nobody.
That is not a failure on anyone's part. The prescribers managing these medications sit in primary care, endocrinology, obesity medicine, and increasingly on telehealth platforms. They are managing a metabolic condition, and they are managing it well. Monitoring changing joint load, spotting early muscle loss, and routing a patient toward orthopedic evaluation was never inside that scope, and it was never meant to be.
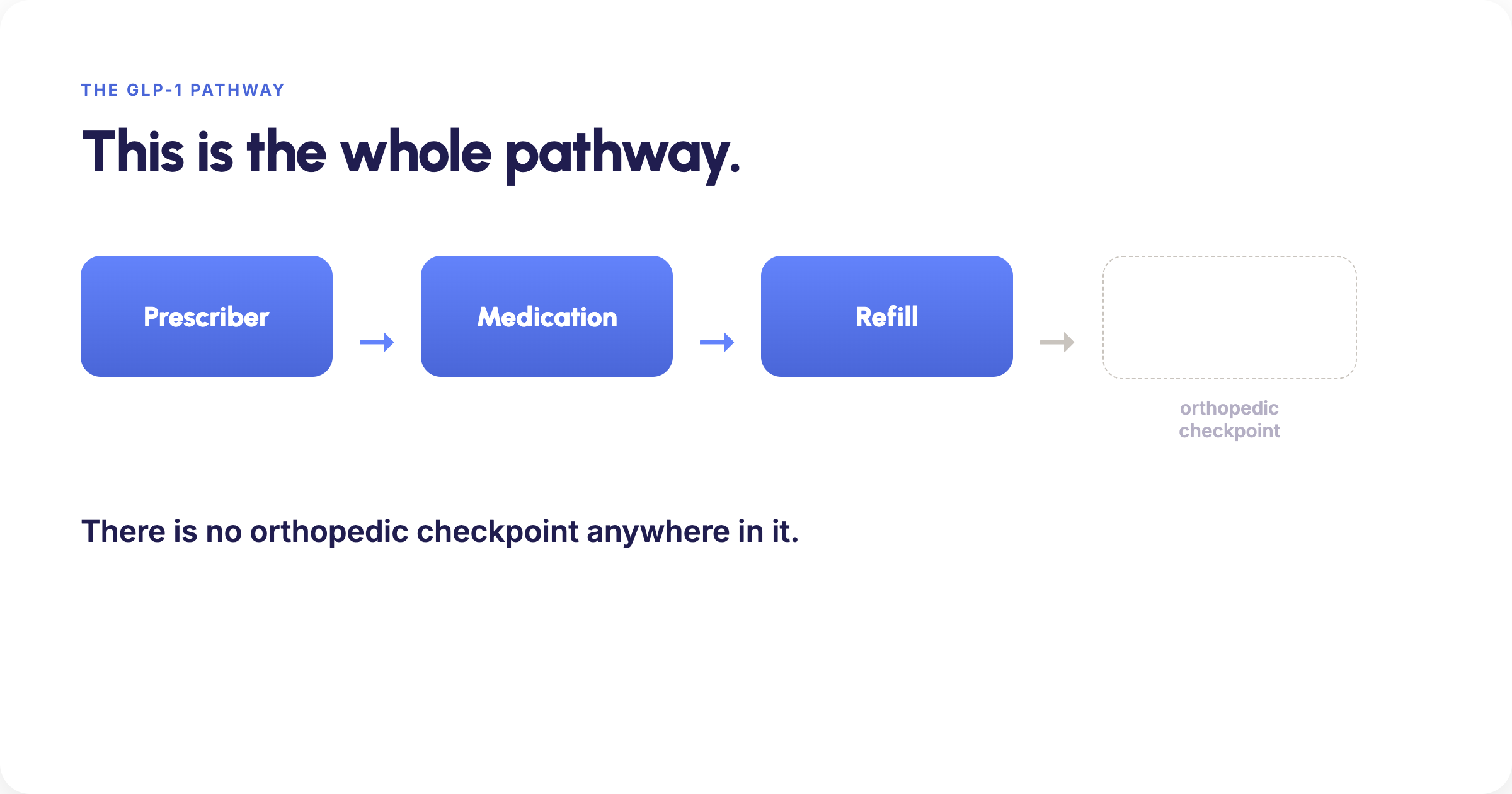
The problem is what sits on the other side. The orthopedic practice has exactly that expertise, and no front door for this patient population. Nothing in the pathway connects the two.
Prescriber. Medication. Refill. There is no orthopedic checkpoint anywhere in it.
The scale of that pathway is worth understanding. A Yale study published in JAMA in July 2026 applied for GLP-1 prescriptions across 49 telehealth platforms. Forty-five wrote the prescription. 91.8% did it on the basis of a self-reported questionnaire and a photo, and 69.4% shipped the medication within 24 hours. That pathway is built for speed and access to the medication, and it delivers both. It was simply never built to carry a musculoskeletal question.
Meanwhile the patient who feels weaker on the stairs, or notices a step that doesn't feel steady, doesn't know whether to wait it out, call their prescriber, or find a specialist. Most wait. Some go to the emergency room. Neither one gets them a real answer.
This is an access architecture problem, and orthopedic practices are sitting on the solution.
What practices can do
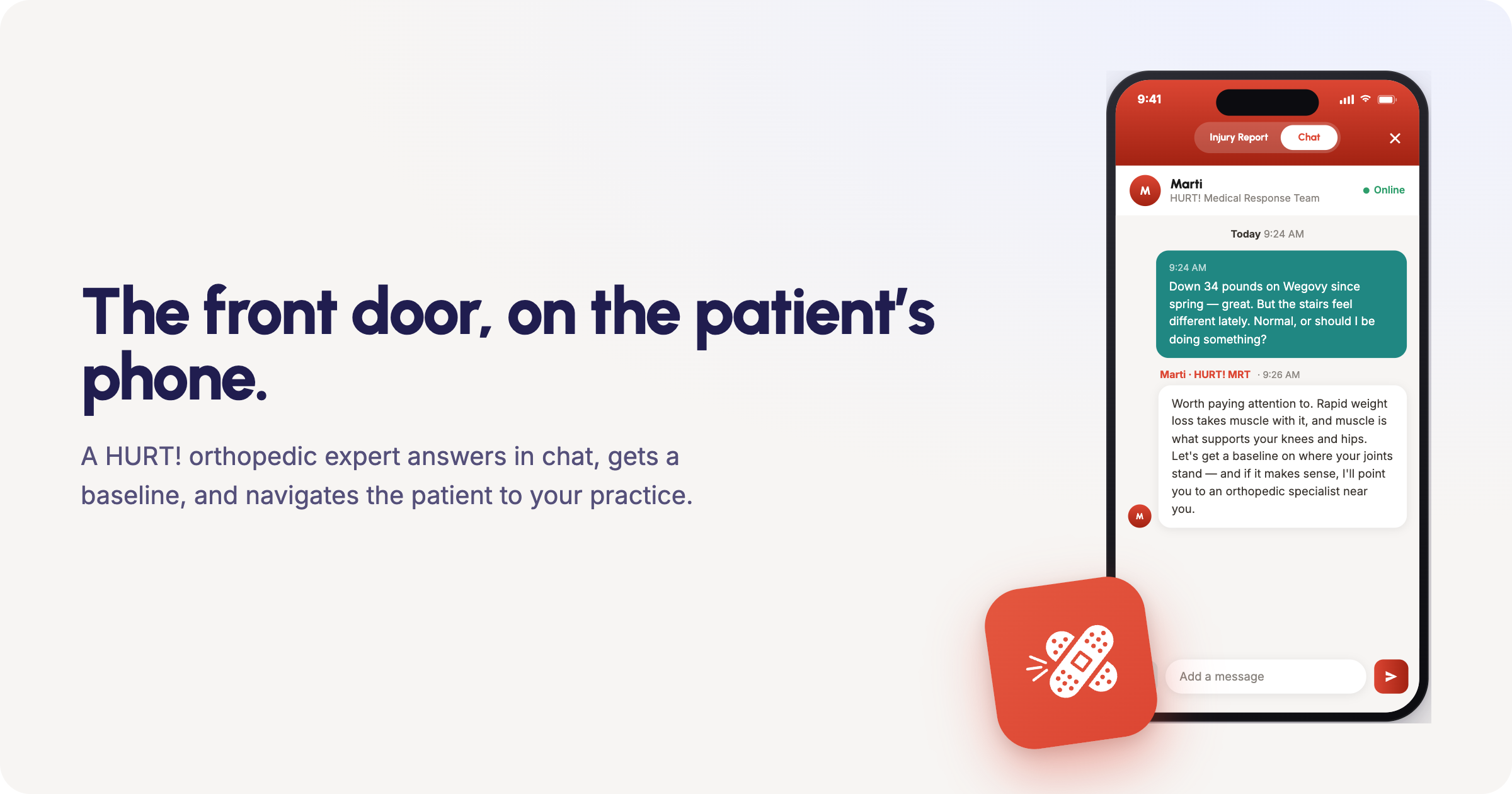
The opportunity is structural. A practice that builds a clear front door for GLP-1 patients will meet a population that currently has nowhere to go. Three things make that door work.
Availability that matches when questions actually happen. A patient notices something at 9pm on a Sunday, not at 10am on a Tuesday. A door that only opens during office hours is not a door for this population.
A quantified baseline. "My joints feel different" is not something a practice can act on. A structured assessment turns that into a number, tracked over time, so a real change is visible before it becomes a diagnosis. That is the difference between a patient who worries and a patient a practice can route.
Data infrastructure that shows the demand forming, so the practice can plan against something real rather than a hunch.
GLP-1 adoption among commercially insured patients has more than quadrupled in five years. The orthopedic volume that follows isn't hypothetical. It's already forming, and it's arriving through a pathway with no orthopedic checkpoint of its own.
Nobody built that door. Build it before the volume finds it closed.
John DeLucchi, PT, DPT, MBA is Director of HURT! Digital Recovery at HURT!, a structured musculoskeletal access platform built inside orthopedics.
Sources
- Springer / Healio: GLP-1 use among commercially insured adults, 2019–2024
- PMC12264624 — STEP 1 trial lean body mass analysis
- PMC12544599 — Endocrine Society: BMD declines on semaglutide/tirzepatide (34-month follow-up)
- JCEM (dgag052) — BMD in non-diabetic GLP-1 RA patients vs. matched controls
- AAOS 2026 Annual Meeting Press Kit — 73,483-patient matched cohort, 5-year osteoporosis data
- Chetty AK, Chen AS, Ross JR, Ramachandran R. Online prescribing of GLP-1 receptor agonists. JAMA. Published online July 6, 2026. doi:10.1001/jama.2026.9131


.png)